 Sign In
Sign In 0 Items (
0 Items ( Search
Search








I have seen a husband caring for his wife—and their four young children—in the last months of her life as she suffered from breast cancer. I have witnessed an elderly woman look after her husband of more than 50 years but who no longer recognised her. And I sat by my own father’s bedside through his final days of palliative care. Each of these experiences was precious, even though they were marked by heartache and loss. As former NSW premier Mike Baird has argued so well, never in the history of the world have we become so adept at palliative care. And yet, the push for euthanasia is now all but complete, with NSW the only state in Australia still committed to protecting those who are most vulnerable.
There is a plethora of reasons why medically assisted suicide is a bad idea. People might try and coin all kinds of politically correct euphemisms, but that’s precisely what it is. Alex Greenwich, the independent MP responsible for introducing the legislation into the NSW parliament recently said:
Without the option of voluntary assisted dying, people who receive bad news about their terminal prognosis live in fear and, sadly, the rate of death by suicide among people who are terminally ill is high.
What Greenwich fails to realise is that his bill wouldn’t reduce this figure while making the option of self-murder all the easier to access. As I have argued elsewhere, to introduce such legislation at the height of a worldwide pandemic in which the elderly are the most at risk is stunning for its audacity. But such is the contemporary moral and political dissonance we are witnessing.
Dr Hannah Graham, lecturer in criminology at the University of Sterling, and Dr Jeremy Prichard, associate professor at the University of Tasmania, have produced an excellent report which outlines the numerous reasons why legalising euthanasia is so problematic. First, the bioethical. At the heart of this issue is the role of medical professionals. In particular, are they healers, helpers or killers? Significantly, a national survey in the United Kingdom has shown that the majority of doctors do not support the practice of euthanasia. What’s more, our own Australian Medical Association (AMA) has also been highly critical of the practice. Dr Christopher Middleton has stated:
I think it would completely change the mind-set and the ethos of medicine in Australia because in their practice, in training, doctors tend to see themselves as agents of hope and healing and comfort, and certainly not as agents of death.
Second, the potential for elder abuse. The European Court of Human Rights put it this way, “…that the risk of abuse inherent in a system which facilitated assisted suicide should not be underestimated.” As Dr Pritchard, in an op-ed writes:
In coming decades we face a rapidly aging population, a shrinking tax base and increases in health problems like dementia…euthanasia could form part of government planning for service provision for people nearing end-of-life…If that sounds far-fetched, consider two cases from Oregon where patients’ applications for medical treatment were rejected, but followed by departmental notifications informing the patients they were eligible for assisted dying.
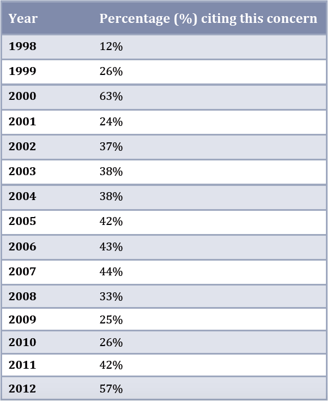 Third, the psychological pressure to end one’s life. Note the table at right, based on statistics from Oregon, which shows that since euthanasia has been made legal in that US state there has been a significant and steady increase in people giving the reason for choosing euthanasia so as not to be a burden on their family and friends.
Third, the psychological pressure to end one’s life. Note the table at right, based on statistics from Oregon, which shows that since euthanasia has been made legal in that US state there has been a significant and steady increase in people giving the reason for choosing euthanasia so as not to be a burden on their family and friends.
Fourth, is the negative societal perception of those who have a disability, with their deaths being treated as an act of ‘compassion.’ Graham and Pritchard writing:
The implication that some people are ‘better off dead’ and that ‘some lives are not worth living’, phrases which have been used internationally in euthanasia debates, are potentially offensive and stigmatising to those who live with the same or similar symptoms and conditions.
Constance Putnam has argued, there is a fundamental problem with framing the issue this way since “a ‘right to die’ is, in a very real sense, a curious concept. To have a ‘right’ to something that will inevitable take place regardless of circumstances or actions – like dying, for each of us – seems odd. As Putnam states, “I can think of no other right that any one of us might have to anything so universally (and absolutely predictably) inevitable.”
Fifth, is bracket creep. What has been observed in countries that have legalised euthanasia is that the wishes of family members have pressured the patient to be choose to be euthanased. What’s more, there is widespread under-reporting of the practice, and there has also been a significant increase in the use of ‘terminal sedation’ resulting in the patient’s death. For instance, Dr. Philip Nitschke, one of the leading proponents for legalising euthanasia, has been quoted as saying:
In the intervening 16 years since the Northern Territory Rights of the Terminally Ill Act came and went, the debate on voluntary euthanasia has been extended beyond those who are terminally ill, to include the well elderly (sic) for whom rational suicide is one of the many end of life options.
Sixth, the ‘safeguards’ of psychiatric referral and assessment are gradually ignored. Graham and Prichard state:
In the Flanders region of Belgium approximately half of euthanasia cases are not formally monitored as doctors do not report them to authorities. The rate of underreporting in the Netherlands appears to be between 20%-23%.
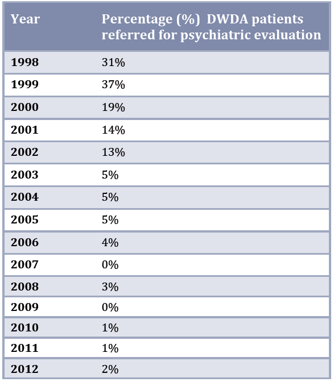 What’s more, in Oregon the percentage of people being referred for psychiatric evaluation has dramatically decreased, as can be seen in the table at left.
What’s more, in Oregon the percentage of people being referred for psychiatric evaluation has dramatically decreased, as can be seen in the table at left.
Seventh, is the eventual practice and acceptance of non-voluntary euthanasia. In Belgium, where euthanasia has been legal since 2002, it has been observed that people were put to death without their consent. Similarly, Holland has now introduced legislation to euthanize patients suffering from dementia without even their verbal consent! What’s more, nurses have taken upon themselves, without the presence of a doctor, the responsibility of administering euthanasia drugs.
Eighth, numerous countries have examined and rejected it. No country should feel that it is on the “wrong side of history” in rejecting this practice when the majority of countries around the world have decided against its legalisation.
Ninth, is the associated guilt when a medical professional is involved in ending another person’s life. For instance, Dr Kenneth Stevens, after researching this particular aspect, makes the following finding:
The physician is centrally involved in PAS and euthanasia, and the emotional and psychological effects on the participating physician can be substantial. The shift away from the fundamental values of medicine to heal and promote human wholeness can have significant effects on many participating physicians. Doctors describe being profoundly adversely affected, being shocked by the suddenness of the death, being caught up in the patient’s drive for assisted suicide, having a sense of powerlessness, and feeling isolated. There is evidence of pressure on and intimidation of doctors by some patients to assist in suicide. The effect of countertransference in the doctor-patient relationship may influence physician involvement in PAS and euthanasia.
Tenth, there are gendered risks, especially for women. There is a growing body of academic literature which highlights the ‘disproportionate victimisation of women’. As Prichard and Graham explain:
It is vitally necessary to carefully consider the potential for gendered violence and familial control to be directly or subtly influential, if not implicated, in matters of the ‘voluntary’ assisted death of women. Where there has been coercion, control and gendered violence in a woman’s life, the nature of which may often be kept hidden and secret from others (including in professional and personal relationships) in her life, it is important to ask whether this might be a factor in a woman’s death.
All of which should make one stop and ask the question, “How would I like to be treated?” As a financial burden? A personal inconvenience? Or with love, respect and dignity. Especially when you are at your most vulnerable in your hour of greatest need. Euthanasia is not an act of compassion but, on so many levels, the crudest form of cruelty.
Mark Powell is a Presbyterian minister

It’s really simple. Whenever has sidestepping a problem been called “dignified” Die with your boots on, however it comes. That’s real dignity.
Katzenjammer – If you are incapable of feeding yourself, sitting up, talking, or any of the other characteristics we relate to a human it is extremely upsetting to your relatives who have known you all their lives as an intelligent, helpful aunt to see that a society that thinks treatment keeping you like this is the least bit acceptable. Dignity has been thrown out the door by this society.
Maxpart27, get over yourself, you’re not the same as you were as a baby, or even as an adolescent.
As I said to you before ,instead of killing them , why not try and be gentle and show some kindness, by helping them sit up or assisting them with their personal care needs.
Good palliative care is the only way to go, showing love to people makes them feel some sense of worth and it makes dying and letting go easier. I remember my grandmother’s death with fondness, my brother simply said to her, “ grandma I’ve now got a baby daughter , her name is Sophie-his final words followed “ grandma we love you” , and it was with those key words that God accepted her life into his care.
Palliative care is therapeutic in that it gently takes people to meet their maker, it also gives them time to adjust mentally, to their impending death, and it also gives the people around them time and contemplative space to adjust and accept this reality themselves. It also gives people the time to orientate their thoughts to their heart’s. Dying and death is a grieving process and by natural law reasoning this takes time, does it not!
Palliative care is therapeutic for all involved, the dying, the family , the nurses and doctor’s ( trust ,matters).
If you look at Mark Powell’s figures on psychiatric evaluation it tells us the initial intent of Euthanasia at face value – the introduction- is the appearance of an ethical death, however once introduced and entrenched ,the real intent becomes apparent, in that ,medically ,fewer and fewer people are psychologically and psychiatrically assessed, the aim and intent is industrious, to kill people with complete indifference to medical condition or treatment- in other words if you want to kill yourself ,we’re happy to facilitate that, as part of a clinical business transaction- they don’t care- how on Gods earth is that a sign of dignity Maxpart27?
Dying is a part of life ,we in the West have immortalised living ,and seem to have insulated our lives from the former reality because in large part we have turned our backs on the unpleasant truth about life and living as is known by God – the example of Jesus should be and is the gold standard for living and dying- no doubt.
Whether you know it or not ,putting forward the ideal excuse that your Aunt would be better off dead because you feel uncomfortable, is not good enough, only feeble mindedness, it is also self centred and is no reason what so ever for killing someone, the focus is on you, because you are having trouble coping with the reality of the disease process , I empathise with you – it’s not an easy thing to accept, but accept we must.
Life itself is a sexually transmitted disease (STD) that too lesser or greater extent we are all dying from, at the point of birth.
Dying is easier when you accept acts of love, trust me on this ,if nothing else ,I have been there many many times. Euthanasia is not the answer,as, and it is certainly not dying, more akin to killing, and by implication is not even remotely dignified.
Palliative care delivers dignity in death…….because it is coupled to the key ingredient to living and life – caring love ,that dwells in the human heart.
Lastly and just as importantly is the personal autonomy of doctors and nursing staff, why should they be made to act out premeditated murder on someone else’s behalf.
Maybe what should occur is that those politicians or people like yourself who advocate for Euthanasia should be the ones contracted by the state to practice it, instead of palming off the unpleasant reality to someone else.
The medical professions intended purpose is to care for ,and look after people, not kill them.
As mentioned earlier ,get the politicians who facilitate laws to kill people, to be the ones to do the killing at the coal face, not well educated ,ethical caring compassionate nursing staff and doctors.
As Archbishop Anthony Fisher said, “ what is needed here is better palliative care”,
and the funding for it ,you mean spirited lazy political people ( animals).
STD, I couldn’t agree more. Nor can I think of a single credible counter argument. Watching my brother in his final weeks of a painful illness, he was immensely amused by his family and friends helping him plan the most outrageously extravagant “wake”. We were in no doubt whatsoever that despite his frequent bouts of severe pain, he didn’t need anyone to assist him to die, and the very concept was unthinkable.
Despite all that it is dressed up as the clamour for PAS is a mark of the inconvenience of human frailty for the modern narcissist.
If we are to have euthanasia,one safeguard should be that if a family member encourages euthanasia,they should forfeit any benefit under the deceased’s will.
Following up Andrew Denton’s article in The Daily Telegraph, I wrote to GoGentleAustralia thus:
.
Andrew Denton wrote: “All he wanted was for someone to help end his suffering so that he could die in peace with dignity, which is what he deserved. Surely we can do this for our terminally ill loved ones.”
.
My father died in peace and dignity without any new government laws.
.
My father chose to leave the family home where he was receiving palliative care, including a morphine pump and a daily visit from a nurse, to die in hospital. He could not take food or fluids by mouth and in consultation with the doctor and his wife, my mother, decided to stop the nasogastric intubation feeding that was prolonging his life.
.
I was present but offered no opinion and took no part in the deliberation other than explaining things to my mother when necessary.
.
The morphine pump seemingly kept him pain free – he had his “silly grin” as he lay in bed with family with him at all times, dozing off, waking, looking around to see who was there, grinning, dozing ……
.
Mother and one of my sisters stayed full-time in the room, the rest of us, children, in-laws and grandchildren, spent much of our free time there. But not for long, he died of thirst (maybe helped along by the level of morphine) during his 3rd night in hospital, about 65 hours after ceasing the NG tube feeding.
.
My reading suggests that was not an atypical time for a patient in poor physical condition to die through dehydration (you can last much longer without food but still drinking) – a very good mate, early 60s, in seemingly good nick (tradie, jogger, gym junkie) had a stroke and lay on his back for 4 days in an iron shed in the tropics before being found and the doctor reckoned one more day could have seen him gone and two would have.
.
If life has become “intolerable”, doing without fluid for a few days, far less time than it would take to get someone else to legally kill you, can’t make life more “intolerable”.
.
There is no law that requires a person to drink or allow another to insert fluid into his/her body.
.
Many people have done it, and all reading I have done suggests that “Dying from dehydration is generally not uncomfortable once the initial feelings of thirst subside”, and that is without morphine.
.
They responded:
***
We are very pleased to hear the passing of your father was a very peaceful one.
.
Unfortunately, this is not afforded to everyone. Palliative care itself recognises it cannot relieve all suffering in a small percentage of patients:
While pain and other symptoms can be helped, complete relief of suffering is not always possible, even with optimal palliative care.
.
This is also evident on our wall of testimonies.
.
Voluntary Assisted Dying is for the terminally ill with a limited life expectancy, whose intolerable suffering cannot be relieved.
***.
Governments can’t even do their fundamental functions particularly well – I don’t want them determining where, when, how and by whom I can be put down, not like a badly injured dog as “pro-euthanisers” tend to cite, but like the many more dogs put down because they are no longer wanted.
Today, according to the ABC the NSW government is going to spend $130 million on mental health to’ tackle suicide.’ I wonder why, when so many of our politicians will also vote for euthanasia. Could someone kindly explain the difference between voluntary assisted dying and suicide?
I know it is easy to talk about such things but, having helped to nurse my mother-in-law in her final months, all I know is that dying is a part of life and a soul journey and when we seek to make it neat, tidy, clinical and quick, we deny and diminish our humanity and our spiritual selves. In a world sourced in the delusion of science and its creation, allopathic medicine, that all can be reduced to the material and mechanical, we are sacrificing the substance of life, the messiness of life, the reality of being human in this world and the potential we have to grow as spiritual beings through our experiences, particularly those which are painful. And, in such a profit and power-driven world, I have no illusions about the curse which could result from what some see as the ‘gift’ of euthanasia. We have commercialised IVF and turned babies, human lives, into commodities so I have absolutely no doubt that Euthanasia would quickly become a profit and power-driven commodity which would soil our souls and betray our humanity. We already have Life for sale with often negative outcomes and Death for sale would be no different. Everything has a price. Life is not tidy, it is not fair, it is not even kind, but it is precious and Euthanasia denies the truth of Life and the truth of Soul and Self.
rosross introduced IVF, so I’ll take the opportunity to again comment on The Australian moderators.
.
Gentle Will’s accepted comment:
.
“A biological parent is one who procreates naturally”
.
My response, REJECTED:
.
“The product of my sperm and my wife’s egg has 2 biological parents, whether the egg and sperm met naturally in the fallopian tube or unnaturally in a test-tube”.
rosross, agree absolutely. I particularly love your final sentence. So true.
rosross, I agree with DT wholeheartedly.
The opinions of the people who died would be more valid than that of brothers, children, others. I don’t care what my sons think, I want it to be my decision, not theirs, and my husband will never turn off the machines.
So I want to be able to call on help when I decide enough is enough.