 Sign In
Sign In 0 Items (
0 Items ( Search
Search








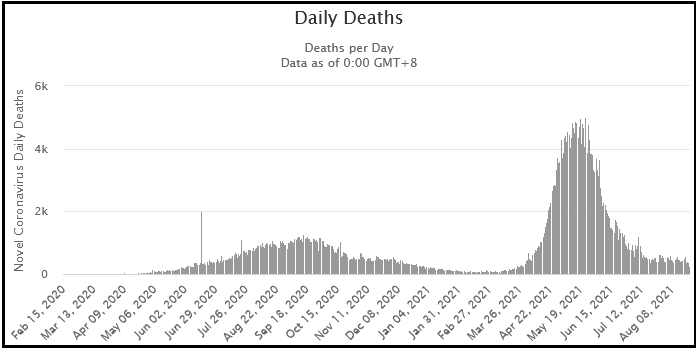
Back in April 2020, the catch phrase was “flatten the curve.” The public was told that without lockdowns, hospitals would be overwhelmed with COVID-19 cases. Hospitals were not overwhelmed, and emergency facilities erected to take care of the epidemic went unused. By September, many jurisdictions that locked down had worse fatality rates per capita than jurisdictions without lockdowns. The goal posts were moved with claims that lockdowns were necessary to avoid catastrophe until vaccines were developed and distributed. By January, the winter peaks in fatalities were in decline before vaccination programs took place.
Most recently, the goalposts have been moved further with the claim that lockdowns are necessary to deal with the Delta variant. Yet, in India (see the chart below) whence the Delta variant emerged, cases and fatalities have already declined to low levels. In the UK, cases declined before the lockdowns and have slowly risen during the lockdowns. Australia seems to lock down whenever a new case is detected. The following discussion will explain why the predictions were wrong, why no government policy in some cases led to superior results than lockdown, and why new outbreaks emerge whenever lockdowns are relaxed.
The horribly inaccurate predictions, including the infamous Ferguson model, extrapolated fatality rates from hospitalized patients to the entire population, made faulty assumptions about homogeneity of risk, and overestimated growth parameters to reach predictions of apocalypse that justified lockdowns. To understand what went wrong with these predictions, we need to examine the dynamics of how respiratory viruses spread through a population.
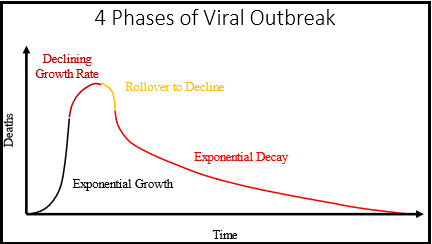
Four phases of a viral outbreak
Phase 1 (Black) is the exponential growth phase where the rate of growth increases with the number of infected persons. Phase 2 (Brown) is the declining rate of growth phase where growth is limited by availability of susceptible hosts. Phase 3 (Yellow) is the beginning of decline where there are still susceptible hosts, but the rate of resolution of cases exceeds the rate of spread to new hosts. Phase 4 (Red) is the exponential decline phase where there are no more susceptible hosts (Herd Immunity), and a percentage of active cases resolve to either death or recovery during each time increment.
Initial models assumed the population was homogeneous with respect to the human host population. By homogeneous, it is meant that the risks of becoming infected, becoming ill and dying from COVID-19 are roughly uniform across the entire population. This assumption turned out to be wrong, but it is necessary to understand the dynamics of virus spread through a homogeneous population before one can understand the dynamics of virus spread through a stratified risk population.
Figure 1 illustrates the dynamics of a viral outbreak through a homogeneous population. For those interested in the maths, the mathematics of viral outbreak are similar to the mathematics of bacterial growth with limited nutrients. There are four phases of growth that transition one to another due to increasing number of infected hosts (cases), decreasing number of susceptible hosts, and resolution of cases to either death or recovery. For a homogeneous population, it is reasonable to assume that the percentage of cases that die will be constant over time; cases are a reasonable proxy for eventual deaths.
Phase 1 is the exponential growth phase. The virus spreads via human contact between an infected person and a susceptible person. As the virus spreads, there are more infected people to spread virus which is the basis for exponential growth. During phase 1, the number of infected people is small enough that decreasing numbers of susceptible hosts does not significantly affect the growth rate. The rate of resolution of cases also increases with the number of cases, but we can assume that the rate of spread is greater than the rate of resolution; otherwise, there would be no outbreak and the virus would disappear spontaneously from the population.
During phase 2, the decreasing number of available hosts becomes a significant brake on the rate of growth; cases continue to increase, but the rate of increase slows. During phase 3, the decreasing number of available hosts is so important that the number of human interactions between an infected person and a susceptible person is no longer greater than the resolution of cases; number of cases reaches its peak and declines. Phase 4 is what is called herd immunity. There are no more susceptible hosts, so the cases decline as they resolve into either death or recovery. This phase follows an exponential decay to zero cases.
Figure 2: COVID-19 deaths per million population from March 1, 2020 until September 1, 2020. Data values are 7 day moving average to smooth out fluctuations caused by weekly reporting of deaths. Data are from Worldometer.
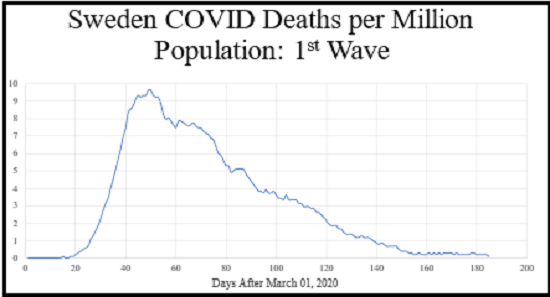
Figure 2 illustrates COVID-19 mortality in Sweden from March 1, 2020 until September 1, 2020. Sweden had very little government policy. The schools were not closed. Restaurants, bars, gyms and other businesses remained opened. There were no mask mandates or official social distancing mandates. Sweden was criticized for this liberal policy, and there were many predictions of doom that did not materialize. As we shall see, Sweden did better than some jurisdictions with government lockdowns. The main features of Figure 1 based on theory can be seen in the Figure 2 real-world data. There is an easily identified exponential growth phase 1, followed by a peak in deaths, followed by a decline approximating an exponential decay to zero. Based on this data, we can infer that Sweden achieved herd immunity to the initial virus irrespective of any measurement of antibody levels. The appearance of an exponential decline to zero is a practical definition of herd immunity.
Effect of lockdown of a homogeneous population
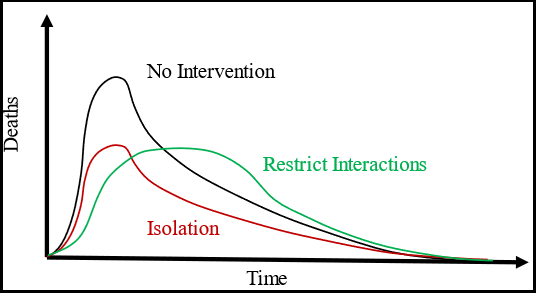
Figure 3: . The Black curve shows the baseline case without any intervention. The Red curve shows the effect of Isolation of members of the population from other members creating a segregated population with non-homogeneous behavior. The Green curve shows the effect of restricting interactions without isolation; the number of interactions for each person is decreased, but each person can still interact. The Green curve is what is meant by “flattening the curve.”
There are two very different types of lockdowns that can be applied to a homogeneous population. One type is to segregate people from each other. This limits the spread of virus to only the members of the cell where the virus enters. There is no interaction from one cell with another, so the other cells are protected. A homogeneous population has been transformed into two groups: one group is at risk for the virus; the other has no risk. In effect this type of lockdown limits the number of available cases which scales the growth curve down in size. The peak occurs at the same time, but the magnitude of the peak is decreased.
An example of this type of lockdown would be decreasing the size of nursing homes such that fewer residents live in a greater number of homes. The other type of lockdown is restriction of interactions without segregation. This limits the rate of spread. This slows the rate of exponential growth, delays the time to reach the peak number of cases or deaths, but the area under the curve (total deaths) is unchanged. An example of this type of lockdown is restrictions on the number of interactions people can have. Closing restaurants, bars, and other businesses is an attempt to achieve this result, but whether the number of interactions decrease or are shifted to other locations is questionable. We can now examine the real-world data to see what the effects of policy were. (Note: I am not trying to predict anything as I do not know the values of the various constants in the equations. Rather I am using qualitative analysis to examine what happened in various jurisdictions and explain why the data looks the way it does.)
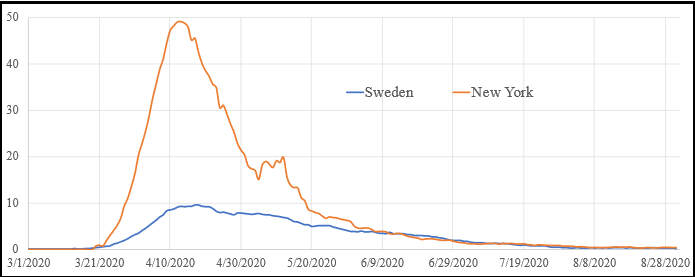
Comparison of mortality data of New York state and Sweden. Data values are 7-day moving average of deaths per million population. Data are from Worldometer. Blue curve shows data from Sweden. Brown curve shows data from New York.
New York state has had relatively harsh lockdowns since the beginning of the COVID-19 pandemic. Governor Cuomo has been very vocal in his criticism of other leaders who did not follow his “lead” in policy. The data show that Sweden, without any formal lockdown, had roughly 20 per cent the mortality as New York with its lockdown. Furthermore, the pattern of the data show that the New York lockdown resulted in a faster growth phase, same time to peak and similar decay pattern as Sweden. We can conclude that Sweden, without any government policy, had superior isolation of people than did New York, where government was actively trying to limit spread.
One explanation for the New York data was the policy that nursing homes could not refuse COVID-19 patients from hospitals. This led to introducing COVID-19 into a greater number of cells than occurred in Sweden, where people relied on common sense. There is no evidence from the data that the closure of schools, restaurants, or bars had any impact on the spread of COVID-19 in New York. This finding illustrates a flaw in the logic of lockdowns. It was assumed that by closing schools, restaurants, bars, and workplaces, that there would be fewer interactions between people. However, it is quite possible that people forced to stay at home will have greater interactions, but with a smaller number of people. We will return to this point after discussing the importance of stratified risk.
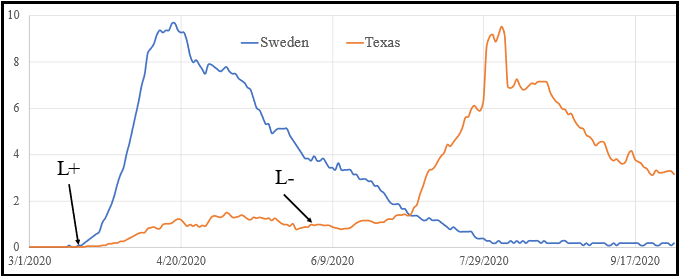
Figure 5: Comparison between Sweden and Texas state from March 1, 2020 until October 1, 2020. Data are 7-day moving averages. Blue curve shows data from Sweden. Brown curve shows data from Texas. L+ indicates the start of the Texas lockdown on March 19, 2020. L- indicates the start of Reopening Phase 3 in Texas on June 3, 2020.
Some jurisdictions did “flatten the curve.” My home state of Texas locked down on March 19, 2020. Restaurants, bars, gyms, and many businesses were closed. Figure 5 shows that COVID-19 mortality had a slower rate of growth in Texas compared to Sweden. Furthermore, the peak of mortality occurred later in Texas (sometime in May). Note, however, that unlike Sweden, the Texas curve did not decline to zero. Rather there was a decline to a positive asymptote or plateau. I will discuss the importance of this plateau further when discussing the dynamics of viral outbreak with a stratified population. Following relaxation of the lockdown on June 3, deaths increased in a pattern very similar in shape and magnitude to what occurred earlier in Sweden. The effect of lockdown in Texas, after the lockdown was relaxed, was a deferral of deaths rather than a prevention of deaths. Note that following the peak on this graph, deaths did not decline to zero in Texas. As a result of this “plateau of death” the total mortality in Texas has exceeded the mortality in Sweden which had no lockdown.
It would appear, therefore, that not only did lockdown fail to prevent deaths in Texas, but the lockdown may also have increased the total number of deaths due to side effects of delay. These side effects are due to stratification of risk in the population and different effects of lockdown on the different risk groups.
Stratification of Risk
We now know that the population is not homogeneous with respect to risk of death from COVID-19. The latest Centres for Disease Control, which include the recent Delta variant outbreak, show that the risk of death from COVID-19 is 600 times greater for someone 85 years of age or greater compared with someone aged 18-29. This stratification of risk requires several important changes in analysis.
Stratification of risk: In contrast to a homogeneous population, there are two groups of people with different risk of COVID-19. On the left are the young people who have a low risk of death. On the right are the elderly with a high risk of death.
We can no longer use cases as a proxy for deaths, because the percentage of elderly cases accounts for the vast majority of deaths. To simplify analysis, consider the situation where the young people on the left have zero deaths. In this situation, cases of young people contribute nothing to the death total. Rather than restricting interactions among young people, the correct strategy to minimize deaths is to increase interactions among young people, and control interactions between elderly people (segregate the elderly) and decrease entry of cases from the young population into the elderly population. An increase in interactions among young people leads to herd immunity faster, so the risk of transmission from young to elderly has a shorter duration of time.
Effect of Lockdowns of Low-Risk Population
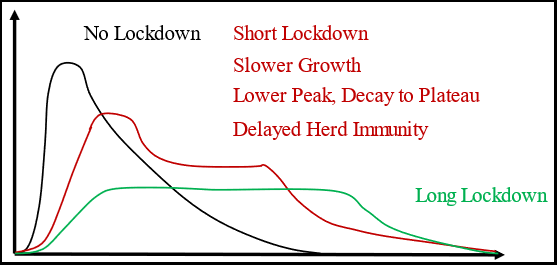
Figure 7: Response of stratified risk population to lockdown of the low-risk group. The Black curve is the situation without lockdown. The Green curve is the situation with a long lockdown (longer than the time for cases to decline in the no lockdown case). The Bed curve is an intermediate result of a short lockdown.
Figure 7 illustrates the expected mortality curves for lockdowns of young low-risk people in a stratified risk population. The Black curve is unchanged from the homogeneous population. This curve is produced by a rapid spread in the young low-risk group leading to a pulse of high amplitude and short duration. As the durations decrease with higher amplitudes, the mortality curve looks more and more like the impulse response of an R-C network. Using signal-processing analytic techniques, as the spread through the young low-risk population becomes lower amplitude of longer duration, the mortality curve looks more like the step response of a R-C network. The Green curve illustrates such a response. Rather than having a fast rise to a sharp peak, there is a slower rise with exponential approach to a plateau. The plateau continues until susceptible people in the young low-risk group are exhausted; the curve then descends to zero consistent with herd immunity.
The Brown curve is an intermediate result from a short duration lockdown. The increase in deaths is slower than the Black curve, the peak is lower than the Black curve, the descent is to a plateau rather than zero until susceptible young, low-risk people are exhausted and herd immunity occurs. Under ideal circumstances, the areas under the curves would be equal, all consistent with the same number of young people transmitting cases to the elderly high-risk group. However, there is difficulty in maintaining precautions for interactions between the young and elderly people over long periods of time. It is possible that alert fatigue will defeat the intentions of the lockdown and more elderly people will be exposed and die.
A very conspicuous difference between the behavior of a homogeneous population and the stratified risk population is the presence of a “plateau of death.” These deaths continue at some nominal level long after the peak has occurred. This plateau is due to slow introduction of new cases into the elderly high-risk population from the young low-risk population long after the cases and deaths decline. The plateau continues until the availability of susceptible hosts among the young people are exhausted and herd immunity is achieved. These plateaus can be seen in many data sets. A very notable example is France, but we can also see this effect in India.
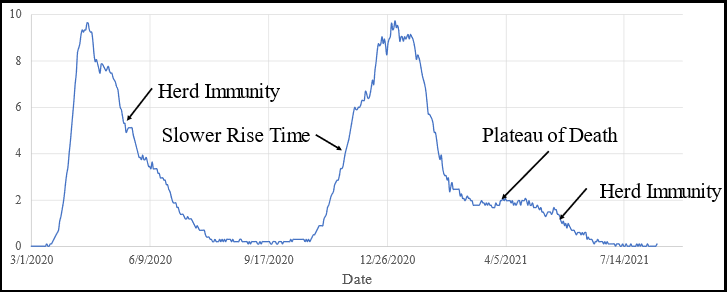
Figure 8: Mortality curve for Sweden from March 1, 2020 to August 11, 2021. Data are 7-day moving averages.
Figure 8 shows that even voluntary restriction of interactions among young people that slow the spread of virus through the young low-risk population can produce a plateau of death by delaying herd immunity. The response to the winter outbreak in Sweden demonstrated a slightly slower rise time during the growth phase, and a very prominent plateau of death prior to the eventual exponential decline to zero after herd immunity was achieved.
Think of it this way. When I was a young boy, the community response to a case of mumps or measles was to have a neighborhood party and put all the susceptible children in the same room as the infected child. All the children got sick at the same time, and the outbreak was over in 3-4 days.
Variants
Why, if herd immunity was achieved in Sweden in the summer of 2020, was there a winter outbreak? The virus adapts to its environment. The virus mutates over time. If the environment selects against certain configurations, mutations that sufficiently change the configuration to fool the human immune defenses grant a survival advantage and the new strain quickly becomes the dominant strain. The winter outbreak seen throughout the world was due to new strains. The current outbreak is due to the Delta variant which has emerged due to immunity against wild type conferred by either vaccine or recovery from illness.
This adaptation is why we have not eliminated influenza despite 100 years of trying. We will not eliminate COVID. Which brings the discussion to the situation in Australia.
What about Australia?
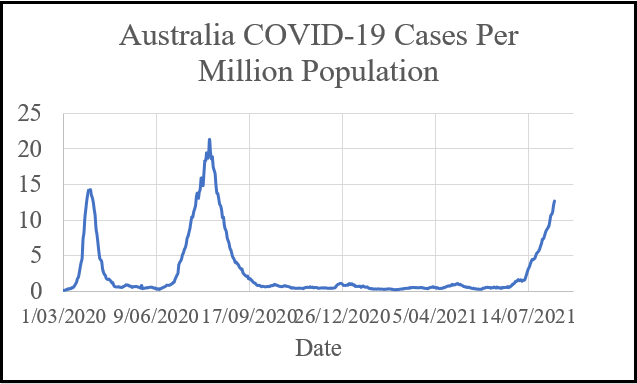
Figure 9: New COVID-19 cases in Australia from March 1, 2020 until August 11, 2021. Data are 7-day moving averages. The graphic illustrates cases, because it is difficult to see the current spike due to the Delta variant if deaths are plotted as the mortality rate is so low.
The policy in Australia has been to lock down whenever a few cases are detected. The mortality rate from COVID-19 in Australia has been very low compared with other nations or US states. However, every time Australia relaxes the lockdown, there is a risk of a new outbreak. This risk will continue until herd immunity has been achieved. As has been the case everywhere else in the world, herd immunity will be temporary. Jurisdictions with extensive mass vaccination programs including Israel have seen outbreaks in cases and the emergence of deaths from Delta variant. Sweden has provided an example of what to expect if a nation learns to live with COVID-19. Sweden appears to be doing just fine.
Australia has a choice to make: either accept that some people, mostly over the age of 80, will die each year from COVID-19; or become permanent inmates in a maximum security prison. Australia was founded as a prison colony. Do Australians wish to become once again a nation of prisoners?
Dr Gilbert Berdine MD is an associate professor of internal medicine at the Texas Tech University Health Sciences Center (TTUHSC) and a faculty affiliate with the Free Market Institute. Dr Berdine earned his undergraduate science degree in chemistry and life sciences from the Massachusetts Institute of Technology in Boston and his graduate medical degree from Harvard University School of Medicine in Boston. He completed both his residency in internal medicine and fellowship in pulmonary diseases at Brigham and Women’s Hospital in Boston. He writes for both the American Institute for Economic Research and Mises Institute and wrote for Quadrant Online on vaping.

This is wrongthink. There is no evidence, in theory, that there is any difference between models and reality.
A number of science-medical experts said just this a year ago and were ignored. We really are run by fools.
rossross.
Fools or those with an agenda?
What is the agenda?
I believe it is the desperate chase for approval of ‘the media’. For a Liberal Government that is a hiding to nothing.
One thing I learned in a career in maintenance engineering is that data is meaningless if it can’t be trusted.
Since the “virus” has never been isolated, the CDC in it wisdom? decided to use a common cold or influenza virus as the reference for the RT-PCR test which, by the way, was totally inadequate for diagnosis. In addition to that, our own TGA declared on it site for health professionals in October 2020 the test is “unreliable and inadequate. Finally, the FDA declared in July of this year that it would with draw the EUA for the test. This renderes the data produced with this test, and therefore the “cases” is completely and utterly useless.
But the politicians insist on reliance on this idiotic data for the purposes of policy and quarantine.
There are really only two possibilities, The political class is completely ignorant and useless, or there is another agenda that has nothing whatever to do with the health and wellbeing of the population. This “other agenda”, given the proclivity of the elites for population reduction, and the earlier forecast by the CIA related Deagel.com., as well as the efficiency with which the injections (those that are mistakenly called ‘vaccines’ kill and maim, is becoming glaringly obvious. The slavery of the police state defined by the WEF as the “Great Reset” depends on a drastic reduction in population. Deagel reckoned this to be about 50% for the USA, 33% for Australia, and 25% for Canada. To maintain this, the injections target the reproductive organs of both sexes.
It’s wakey wakey time.
The thing is we have become fundamentalists. You can make all the predictions under the sun, but unless you can say no one will die under your preferred modelling, no one will listen to you.
As we used to say at school, ‘Define your terms’. Is a ‘case’ a death? Surely deaths are the essential criterion. Some 400 people die each day in Australia of all causes. To me, the ‘Australia Covid Cases Per Million’ graph is very misleading.
A really important contribution to at least shine some small light on what has been missing in the whole (note with a ‘w’) egregious totalitarian response to the Wuhan flu. It was always critical that we quickly came to grips with what the inherent nature of an airborne respiratory SARS CoV-2 virus is, and how that nature would interact with ours. It seems, as many argued early on in this pandemic, that Sweden had most calmly and methodically made the most insightful and wise course of action in the face of that challenge. We have many proxy respiratory diseases on which to make some very good observations on the population wide, natural history of coronaviruses and similar viruses such as influenza and rhinoviruses. The cool calm observations of the article here are the discussion that should have been taking place, away from the Ferguson model, by all health bureaucracies 18 months ago. What must never be forgotten about this virus, from a now insurmountable body of evidence, is that it is inherently a mild virus in its propensity to illness, where that does develop, however it is the immune challenge it represents due to its novel existence that is why the main cohort for fatality is the already frail. What this pandemic however has shown up, is a very grave illness indeed in our political and bureaucratic class that carries with it far graver concerns than a novel cold.
Look at the bright side of all this- the enforced practice of mask wearing has put us all in good stead for when Labor returns to power and we start bringing in 700000 units of consumption into the country per year.
The compulsion of mask wearing makes the possibility of vertically integrating the importation of exotic diseases such as tuberculosis into the immigration mix- as well.
If realised this left wing human rights wishing well will ultimately lead to sustained and higher share yield, prices and profit which will allow governments of all persuasions the possibility and probability and excuse for reintroducing capital gain tax with death tax incentives, in order to sustain and pay for the COVID social experiment-LUNACY
Here is a real life fairy tale that we are living today.
https://off-guardian.org/2021/08/22/the-vapor-the-hot-hat-the-witches-potion/
Yes, “Australia has a choice to make.” But who is going to make it? As a Victorian, I don’t see our Premier (affectionately known in my household as ‘Big Ears’) ending restrictions any time soon. He’s already pointing out that even were we to get to “70 and then 80%” vaccination rates, nothing will change unless at the same time case numbers are low.
The only way case numbers will be low is if the vaccinated don’t get tested. The unvaccinated 20% can probably be relied on not to be compulsive takers of tests.
So we need the utmost faith in the efficacy of the so-called vaccines. Strange days.
Read it carefully, for it clearly explains the theoretical basis of herd immunity, and shows some of the flaws of extrapolating from models using often imperfect data and flawed assumptions about age and other population stratifications. Flawed assumptions also exist by not recognising that individuals, given responsibility, make their own judgements on risk and behavioural adjustments re managing it.
Implicit in the biology of the epidemic curve is an assumption that pathogens will do what we expect them to do, and become driven by evolutionary processes to become more contagious but less virulent. Sadly, pathogens don’t always do that was they operate within many environmental arenas (especially during a world-wide pandemic) and so variants emerge; some of them highly opportunistic.
Classic Red Queen stuff. Our immune systems are lucky if they are one step ahead all the time.
Politically and socially, the only pathway ahead for Australia is to open up from lockdowns at a set rate of vaccination. Where that number is set depends on how much and what sort of pain we are prepared to accept in terms of morbidity and mortality as well as whether political boldness or timidity wins the day. Our freedom percentage might be easily set at a lower figure if we had slowly developed some natural population immunity to this disease, but our eradication strategy, purchased at very significant cost by lockdowns, has meant that we may struggle to keep hospitalisations down in our unexposed population some of whom, unvaxed but older, will remain very vulnerable. That’s unless those at great risk get cautious, plus as a nation we get lucky, so that the virus attenuates well, and summer days keep us outdoors and full of Vitamin D3. Then we might hardly note this ‘epidemic’ in its passing, as it retreats into being simply another endemic respiratory virus that we can conquer, like influenza, with a regular booster vax for the at-risk population. Fingers crossed for that ‘lucky’ version.
What choice? Since when have we had any say in this? There is no choice, we’re just doing what we’re told by people with pepper spray and a legal system that no longer regards people as meaningful.
‘To understand what went wrong with these predictions, we need to examine the dynamics of how respiratory viruses spread through a population.’
I disagree. What we need to understand is why is is possible that such criminal, dithering incompetence is allowed to advise and direct major public policy.
It’s time to end the farce of mask-wearing. Here’s a link to an excellent scientific paper on masks and their lack of fitness for purpose.
https://www.technocracy.news/masks-are-neither-effective-nor-safe-a-summary-of-the-science/
“Do Australians wish to become once again a nation of prisoners?”
YES they do want that. My neighbour assures me that lockdowns are essential and should be accepted willingly because otherwise all the irresponsible idiots in the community will spread the virus. I’m sure the CHO’s, Police Chiefs and Premiers agree with this view, but it is also widely accepted in the community, possibly because the authorities keep repeating it every day in the media.
@Elizabeth B
>”Sadly, pathogens don’t always do that was they operate within many environmental arenas (especially during a world-wide pandemic) and so variants emerge; some of them highly opportunistic.”
Of course viral pathogens follow evolutionary lines. The more successful in terms of infectiousness they become, the less other strains are able to compete for hosts. Of course mutations can be and are opportunistic – this is the very core of evolution. Because the “host” population is not genetically homogeneous in terms of immune system capabilities, complete herd immunity is unattainable, but killing large sections of a “host” population simply means a less lethal but equally infectious strain will compete successfully.
A highly credentialled British immunologist gave a public lecture at Sydney Uni quite a while ago. Following a question from the audience, he related one result from detailed research into HiV. It was noted that certain Northern European populations had a much lower HiV rate than the norm, so the long-term pandemic history of these groups was carefully examined. It was found that ancestral populations from the same areas had also exhibited a far greater resistance to the various Medieval plagues than had been the norm.
Inherent natural immune systems are heterogeneous. The article here from Gilbert Berdine vigorously makes this point to expose the large fault line in current models used for policy. It also incidentally exposes the huge and dangerous lack of understanding in our hysterical MSM, who chase “case numbers” through assumed homogeneity to generate covid-porn clickbait as a business model.
Just watched Frydemeggs on tv wabbling on about States reneging on the 70%-80% open plan.
He’s crab-walking away from it. The Doherty Institute modelling plan is dead in the water.
Never really had a chance against double-crossing Premiers. Daily Telegraph headline “Morrison Govt Refuses to Fund Hospitals, Schools in WA/Vic/SA/Q’ld/Tas”.
Now is the last political nexus for our federal politicians, especially those in government to grow a pair and draw a line in the sand. If it indeed has become the case that the pandemic has been elevated to a National (and of course , international) ‘crisis, how can we arrive at a situation where the state governments run colluded agendas on exercising rigorous compliance measures which have been an affront, to the Australian way of life and the values of the ‘fair go’ ethos. Increasingly what has been leveraged as political capital will soon become a political ball & chain as a substantial proportion of the population, who are increasingly growing frustrated and contemptuous of heavy government edicts, become broadly aware that the virus is endemic globally and is here to stay, and most likely to become less and less lethal, due to both increased immune capacity in its human host and the viruses own evolutionary pathway as outlined in this article.
I’d be interested in a sociological study of our present experience (I mean real sociology, not the marxist fakery we hear about). We are, it seems, subject to two features of the millennials-in-control: abject fear of death for which the responsibility has been outsourced to the government based on the media pump priming we’ve suffered, and unwarranted trust in ‘models’ (whatever millennials think they are). Models, as the saying used to be, are sometimes useful, but always wrong.
I wonder if there are ‘models’ or just one favoured model. I wonder if it includes mental health effects, both short and long term for young people, I wonder if it includes the overall population death rate (that is do CV-19 deaths change the general quantum), I wonder if it includes the general social detriments, educational loss, psychological deprivation, business costs and loss of health arising from peoples’ new found reticence to visit the tele-doctor, or have screenings done.
Or, are we just in the hands of deluded wreckers and manic politicians?
Dear Dr Berdine,
Thank you for your insights! Particularly the plateau of death in Figure 8 due to the delay in reaching herd immunity, which put the vulnerable at risk for longer.
Focusing on Figure 8, may I now discuss this section with you? “The current outbreak is due to the Delta variant which has emerged due to immunity against wild type conferred by either vaccine or recovery from illness. This adaptation is why we have not eliminated influenza despite 100 years of trying. We will not eliminate COVID.”
Assume, as you say, Delta is more contagious (most likely of course).
But also assume, since natural immunity to viruses is almost exclusively due to T cell response rather than antibodies, Delta can be easily recognised by a person who got earlier variants.
Aside notes. (In my understanding):
1. T cells kill a whole human cell if it is invaded by the tiny RNA virus. An RNA virus (such as coronaviruses) depends on the human cell to make more copies of itself.
2. Antibodies are large in size and can kill an actual pathogen such as a bacteria (too large to get into cells and do not need to invade human cells because they have their own DNA )
3. T cells can easily cope with the tiny difference between the different corona viruses. Even the difference between Sars 1 and 2 !
4. Coronaviruses do of course achieve successful mutations, but nowhere near as well as flu viruses.
So, I think we may need a different explanation for the second outbreak in the Figure.
Perhaps consider the following two explanations:
A. The proportion of a population that must be immune for ‘herd immunity’ depends on the ability of the virus to transmit. So, if a new variant is more contagious, even though easily identifiable by T cells, it would require a higher proportion before herd immunity could be reached. This would mean a new swathe of cases would be infected;
and/or
B. Perhaps the Swedish population was divided into regions (or some other sort of sufficiently separated stratification) of smaller populations, and the first outbreak only reached some of those populations, but the second reached others?
Is there anything that can be done through your modelling to demonstrate whether these (or other) explanations are possible?
On the radio yesterday some doctor was relating the ‘terrible symptoms’ of COVID-19 in a daily (hourly) keep-the-fear presentation. I couldn’t believe my ears. It sounded like little more than a mild hangover. That’s what everyone’s afraid of?
.
The term ‘mental health’ has become increasingly prevalent over the years, no more so than now, as people opposed to lock-downs use the term to argue their position. It almost seems as though they are fishing around for a way to describe what this is doing to us but can’t quite put their finger on it.
.
I guess ‘mental health’ is the best-fit humanist term to describe this particular kind of suffering, excluding true illnesses of the brain.
But if we look at the socialist mindset that is really behind both the imposition and acceptance of lock-downs and face nappies, it becomes clear that ‘mental health’ really refers to ‘spiritual well-being’ (in the
full Christian sense, not the New-Age pantheistic sense).
Socialism is the human condition that has its ultimate goal in the crushing of the human spirit through coercion, control and wilful self-destruction. It is the futile longing to be god on the one hand, and the subsequent longing for death on the other. The anger, despondency, worry, loneliness and sense of hopeless helplessness that lock-downs induce are all spiritual ailments. It is the soul that is suffering, not the mind, and the soul is what makes us ‘be’ alive. They are strangling the life out of us.
Modelling – the poorest form of science or Clayton’s science – the science you have when you are not having science. Garbage in-garbage out.
The overall death rate in Australia has declined during the last 18 months. Covid seems to have replaced influenza as the old man’s friend. For the Prime Minister to say that the death from Covid of a 90 year old is “tragic” is nothing short of ridiculous. Death is the outcome of life and it is time to start demystifying death. And I am 85 y.o. and purposefully unvaccinated on the basis that the vaccine is more dangerous than the disease.
The other mysterious thing about the management of this pandemic is that the unvaccinated are being subject to bullying, intimidation and public denunciation by the elitist mouthpieces and the brainwashed. But, if the vaccine is effective, how can the unvaccinated be a threat to those who have been vaccinated?
The answer, of course, is that the vaccine is ineffective, as well as dangerous.
These are dark times indeed!
Interesting. Given your knowledge of the disease, I have a question you may be able to answer.
The risk of dying from Covid seems to triple for each decade of age, yes? So if I get the disease this year, how much more likely am I do die of it than if I’d got it last year?
Bearing in mind that if I’d got it last year, I’d now be immune.